
Urinary Tract Infections in Children

What would you think if your child, who had been toilet-trained for many years, began wetting the bed but was otherwise healthy and in no discomfort; or, if your little girl, 2 1/2 years old, began refusing to sit on the toilet, had a low-grade fever, and was extremely irritable; or, if your 15-year-old boy told you that he had pain on urination for the past four or five days and was now passing bloody urine; or, if your 12 -year-old girl, who had had two or three urinary tract infections in the past, now complained of a backache and began having fevers and chills.
Teen with secondary enuresisAll of these cases represent some of the varied presentations of urinary tract infections (UTI) in children.
The Urinary Tract
The urinary tract is a wonderful waste-removal system. It is, at the same time, simple and effective yet very sophisticated and complicated.
What we call the urinary tract begins with the little balloons of blood vessels in the kidney (glomeruli) which act like tiny sieves excreting excess blood fluids and wastes into the collecting system which surrounds them; but, keeping blood cells and other large particles contained inside the blood stream.
The large “good stuff” and some fluid stays in the capillaries at the sieve; but, much of the fluid, “bad stuff” and even a little “good stuff” gets dumped into the waste collecting system. Then, as all of this fluid makes its way through the many winding microscopic tubules into larger and larger tributaries, the “accidentally dumped” good parts and just enough of the fluid to keep things in balance are reabsorbed back into the blood stream.
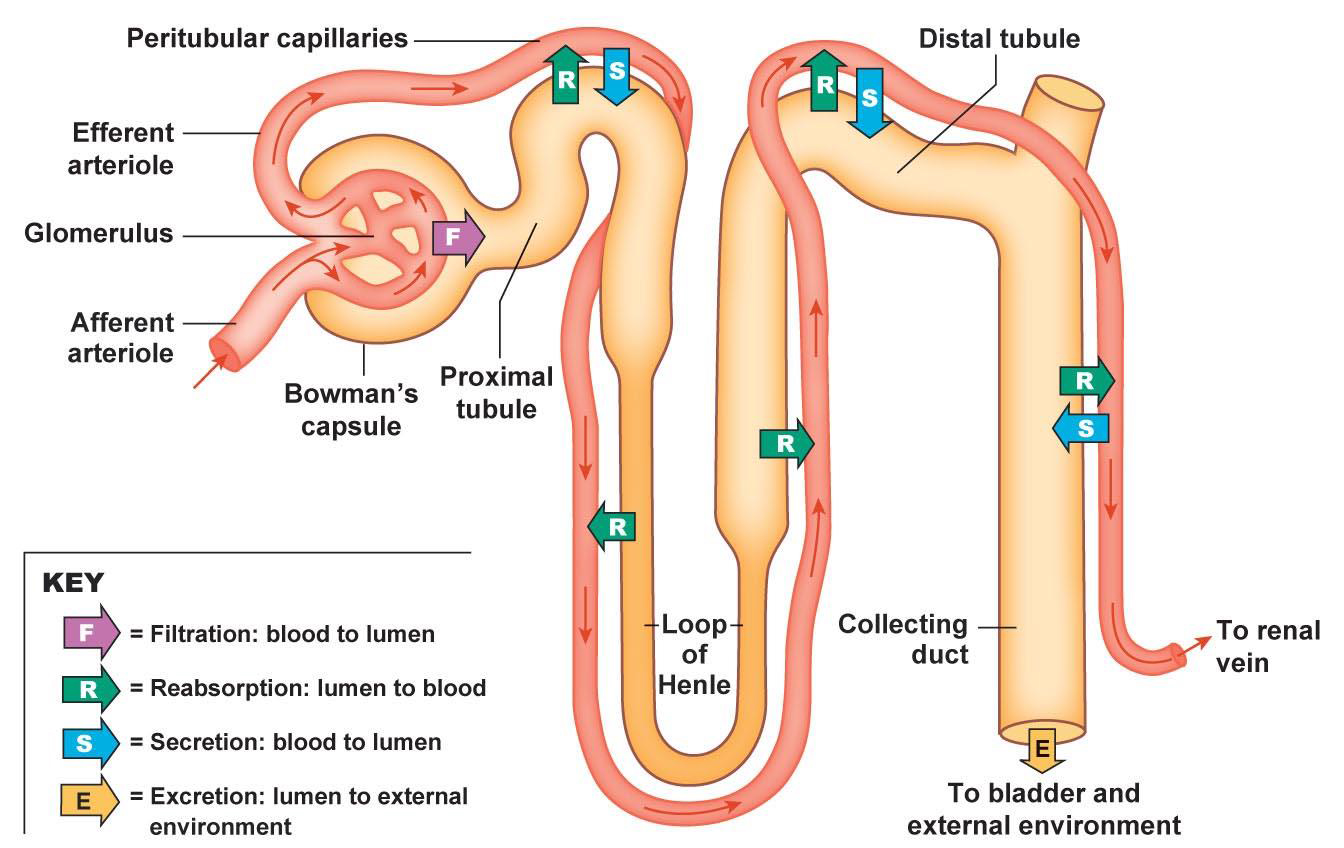 Graphic of kidney tubules and their function
Graphic of kidney tubules and their functionThat leaves the waste material and excess fluid (urine) behind in the tubules to descend down the ureter, from each of the two kidneys, and into the bladder.
Interestingly, the ureter enters the bladder at a strong angle which, when the bladder is full and is under tension, tends to form a flap that acts like a valve to prevent back-flow into the kidneys (neat, huh?) However, it does also cause any new urine being made to back up into the kidney; which is why “holding it” for too long gives you a BACK ache (over the kidneys.)
The urine is stored in the bladder causing it to expand until a complicated set of different muscles both relax and contract in different sequences to force the urine out the urethra.
Urinary Tract Infections
A urinary tract infection can be anywhere along this whole tract — from the kidneys (nephritis) to the collecting ducts (pyelonephritis) to the bladder (cystitis) and to the urethra (urethritis).
Physicians classify the workup and treatment of urinary tract infections into four broad categories: adult and child, which are totally different; and male and female, which are totally different.
In children (especially little girls) an infection can be totally asymptomatic (without symptoms). It is not uncommon for a doctor to find an unsuspected smoldering urinary tract infection, even with late kidney damage, on a routine urine screening for preschool which is why pediatricians routinely screen children’s urine at various times during childhood.
 Urgency, a common indicator of UTI
Urgency, a common indicator of UTIIt is not uncommon for a little girl to have one or two urinary tact infections as she struggles to learn to remember to wipe from front to back, instead of back to front, following a bowel movement.
If she wipes in the wrong direction, stool contamination can result which can cause a vaginal or bladder infection.
Contamination from the bacteria of feces are the most common bacteria in all urinary tact infections. The problem is that there is a very large number of types of bacteria in the feces.
Treating Urinary Tract Infections
If your physician suspects a urinary tract infection, he will perform a urinalysis. If there are pus cells found, he will need to get a urine culture to see for certainty what bacteria is actually causing the infection.
This is especially true if the patient is a child, if it is not the first infection, or, if it’s in a boy. Specialized cultures are obtained in older adolescents who might be sexually active.
An appropriate antibiotic is chosen by your physician (depending upon numerous factors) and treatment continues for about two weeks.
At the same time, symptomatic relief can be obtained by drinking extra amounts of fluid – to thin the urine; and drinking cranberry juice – to acidify the urine.
Little girls may use sitz baths twice a day if they have any vaginal symptoms.
Followup After Treatment
In children, however, the most important part comes after initial treatment. They must be followed up according to the schedule your physician advises.
X-ray studies are almost always done after the first infection in boys, and after the second or third infection in little girls. This is because an infection is a more rare occurrence and therefore much more likely to mean a significant problem in males.
Another problem is that urinary tract infections can return even without symptoms.
My recommendation is to obtain a urinalysis every month for six months after an infection and then at least every year for four or five years.
Other physicians use other schedules, but the principle is that the parent needs to remember to have the child periodically checked if you hope to avoid damage to the kidneys and other organs from a “missed” urinary tract infection. This is because the “second” infection may often be without symptoms, especially in girls but even in boys.
3 Posts in Enuresis-Bed Wetting (enuresis) Series
- Urinary Tract Infections – 9 Apr 2015
- Part 2 - Bed wetting – 6 Jul 2013
- Part 1 - Bed wetting – 9 Jun 2013
Advertisement by Google
(sorry, only few pages have ads)