
Puberty: Tanner Stages – Girls

The original study of childhood growth and maturity done by Dr. Tanner at the Harpenden orphanage in England during WWII has been replicated and verified many times since then.
Growth, development and maturity – a wide range of ages
We now have a pretty secure knowledge that the hormones which produce puberty do so in a fairly consistent manner – even if they don’t correlate but in a very general way to a child’s chronological age. By that I mean: boys and girls follow a fairly well-defined path to physical maturity; but WHEN they start doing it has a very, very wide range.
For example: The pituitary sends signals to begin producing a girl’s puberty-inducing hormones (Stage 1) somewhere in the 4 years between 8 and 11. [In a boy those signals have their start anywhere along the 4 years between 9 and 12.]
Dr. Tanner and Puberty
Obviously, starting the hormones a-flowin’ comes before any actual body morphing is noticeable – which, again, takes another 1 to 2 years, extending the variability even further.
Why is there such a big range? Who knows! Genetics, nutrition and other environmental factors, activity levels, stress, additives and other adulterations in food – all of them are logical and are thought to have some possible undefined effect but nothing’s been proven.
The fact is that the differences between children seen in school classrooms for grades 1 – 4, seem nothing compared to classrooms full of 5th through 7th graders – which become very strange indeed. Some school districts even invented “middle school” to control the chaos.
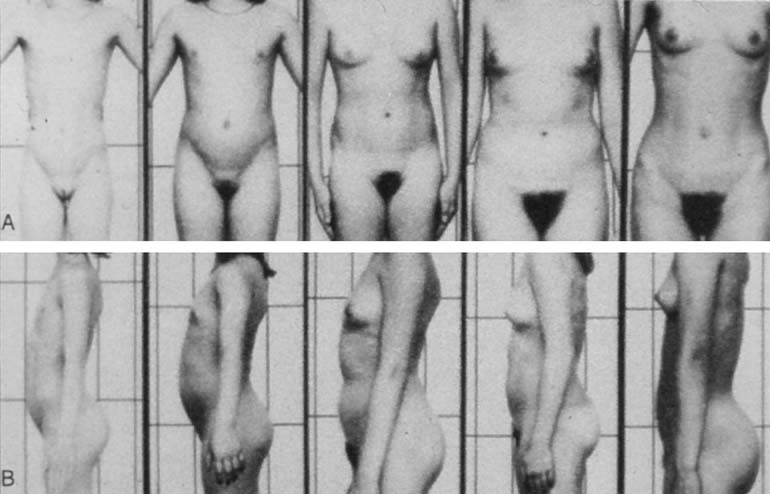
As Dr. Tanner found, if one places serial photographs of several children in successive rows it is easy to adjust the row left or right to match puberty start, and then find that the range of progression through puberty will be shown in successive columns.
He was able to identify five “stages” which are meaningful indicators to physicians about how a child is progressing through puberty, each with their “ranges of normal.”
The Tanner scale then is a scale of physical development in children, adolescents and adults. It defines the specific physical measurements of development, based on external primary and secondary sex characteristics, such as: the size of the breasts; genitalia; development of pubic and axillary hair; and, for boys, testicular volume.
Let’s take a look at the several stages a girl goes through during puberty.
Stages of Puberty in Girls
- Stage One (approximately between the ages of 8 and 11) — This stage begins fairly surreptitiously when the hypothalamus notifies the pituitary to begin orchestrating the puberty process. It can be identified, should one choose to do so, by the increase of various hormones circulating through the blood, which weren’t there all through earlier childhood.
A girls ovaries will enlarge internally, and female hormone production will begin; but external development is not yet visible.
- Stage Two (approximately between 8 and 14) — Breast development is usually the first sign of a girl’s puberty to be noticed. Small buds of breast tissue can be felt just below the skin of the nipple, which may be slightly tender as they start to elevate, and the Aureole (area around the nipple) begins to increase in size.
Stage two begins the height and weight growth in girls too, as their bodies begin heading toward a more adult curvaceous form. Initial growth of pubic hair may be seen which is usually fine and straight before it becomes more coarse and curly.
- Stage Three (approximately between 9 and 15) — Growth in height and weight continues in this stage along with breast tissue. Pubic hair becomes coarser and darker.
Even though not visible, hormonal effect on internal organs are well underway and there may be a whitish discharge from the vagina. Sometimes uterine development has progressed far enough along to generate a girl’s first menstrual period but it’s usually light and is probably not regular.
- Stage Four (approximately from 10 to 16) — If it hasn’t already started, stage four will bring on Menarche (first menstrual period) along with ovulation; but, still it may not necessarily be on a regular basis. Ovulation usually is what makes a girl’s “periods” regular, but not necessarily in the early stages. (It is also possible to have regular periods even if ovulation does not occur every month.)
Other development progresses as well: Aureoles darken and separate into a secondary mound above the rest of the breast and pubic hair extends to a more adult triangular pattern.
- Stage Five (approximately between 12 and 19) All adults are walking around classified as a “Tanner stage five.” Stage five is the final stage of outward physical development and is largely where a girl child has been heading ever since her pituitary got the go-ahead to make a woman. Full height is reached, young women are ovulating regularly, pubic hair is filled in and the breasts are developed fully for the body.
Voice changes have occurred, sweat glands have developed, acne has usually subsided, skin and hair changes have completed over breasts and genitalia and much of the emotional rollercoaster-drama has subsided. She has reached physical maturity; HOWEVER, just like stage five boys, she is not yet emotionally/psychologically mature. (More on that later)
Summary of Physical Findings
| Stage | Breasts | Pubic hair | Height velocity/yr | Other |
|---|---|---|---|---|
| I | Elevation of nipple | Villus hair only | 5.0 to 6.0 cm (2.0 to 2.4 in) |
Prepubertal: no sexual development Adrenarche |
| II | Breast buds palpable Enlarged areola |
Sparse, slightly pigmented | 7.0 to 8.0 cm (2.8 to 3.2 in) |
Breast budding, Body odor, First pubic hair, Height spurt, Clitoral enlargement, Labia pigmentation |
| III | Mammary extends beyond edge of areola | Coarser, darker, curled | 8.0 cm (3.2 in) |
Breasts enlarge, Pubic hair darkens, becomes curlier, Vaginal discharge, Acne, Underarm hair |
| IV | Nipple mound stacked on areola mound | Adult type, but not beyond pubic area | Less than 7.0 cm (2.8 in) | First menstruation, Nipple is distinct from areola |
| V | Integral nipple mound | Adult type, spreading onto inner thigh | Final height reached at age 16 | Fully mature female, Pubic hair extends to inner thighs, Increases in height slow, then stop, Adult genitals |
Issues in Puberty
Timing: Premature Onset
When Dr. Tanner first did his analysis, it was immediately noted that boys and girls had different “timings” in many aspects. Girls began stage 1 pretty much a year or so before the boys – on average. Girl’s large growth spurts were earlier in the stages, largely the first two years, while boys took another year or so to get the velocity up and running.
 Puberty one year earlier since the ’50’s
Puberty one year earlier since the ’50’sThat was in the 1940-50s. Then there came the more industrialized, mechanized, computerized, nutrition-ized years leading to now, when we are noticing that Tanner stage 1 is beginning almost a year earlier across the board!
Why? Another unanswerable question. Less stress? Perhaps. More abundant food? Probably. Immunizations resulting in comparatively disease-free childhoods? I would guess. Injected/added hormones to food? Could be. Microwave towers, increased electro-magnetic radiation or a thousand other things unique to our 21st century culture? Likely.
The fact is, these days the “new normal,” for when we would consider doing a medical workup to look for problems in girls, is: breast development before eight, and first menses before ten. I can tell you however that, even though us medical types see it and know it’s occurring, much of the general public still does a double-take at an eight-year-old with breast tissue forming or a ten-year-old starting her periods.
In fact, still today the majority of parents pretty much put off their “puberty talk” as long as they can get away with it – if they do one at all – which means menses at 10 catches many parents (and girls) off guard. The substantial growth spurt right out of the gate with breast development, does tend to give parents of girls a bit of a heads-up, however.
Why do we bother with all this timing stuff? Well, because there are some pretty severe medical problems that cause puberty to be out of whack, many of which can be treated if caught early, but which are very costly to work up.
Excess hormone from somewhere, either from the brain or gonads and adrenals due to tumors or genetic diseases, is the cause of early puberty. Brain injuries or infections can also stimulate the early onset of puberty.
The pubertal process is so hormonally complicated that there are often more than 10 which need to be analyzed by blood tests individually. Tumors require x-rays, CT scans or MRIs, not to mention thorough physical examinations and meticulous clinical histories in order to piece everything together.
Treatment, if possible, may require surgery or in some cases one of the new medicines developed to counteract an excess hormone.
Timing: Delayed Onset
There is an “earliest” normal time for the onset of puberty. Is there a “latest” normal time too? Yes, although most of us hedge our bets here too, especially in active girls.
No breast changes before thirteen, or no menstrual periods before fourteen are considered the upper limit where a physician can “watch and see” before undertaking some diagnostic studies. We hedge our bets a little here too, because it’s actually quite common for competitive girl gymnasts, dancers and other athletes to not have their periods. Even those who have already begun menstruation and then become athletic may stop or become irregular.
 Progression from girl to woman
Progression from girl to womanDelayed puberty is due to insufficient hormone. If the pituitary output is inadequate, so will be the output from the gonads and adrenals. Like I said the “system” is a bit complicated with one hormone acting on another and others slowing down or inhibiting still others in order to keep everything in balance.
To diagnose where the problem is located, doctors “follow the chain” to see where the “blockage” is coming from. For example, if some genetic disorder is preventing a hormone “down the line” from being made, the pituitary senses things aren’t happening so ramps up its secretions so things will go faster. If we test for the pituitary hormone and find that it’s high, and the hormone down the line is low, then we might surmise that it may be validating our assessment that the problem is coming from one of the steps further down the line.
Depending upon what we find is the cause, these days we have synthesized hormones that we can inject which will both start and maintain puberty long enough to cause the change from a child into an adult. We don’t like to delay treatment because necessary bone growth is also affected, not just the genitals and breasts.
Abnormal Hormone Production
Additionally, for females, there are abnormalities in hormone production which can produce male characteristics such as hair patterns, voice changes, muscularization and clitoral enlargement. These are known as “virilizing” syndromes and can occur in a girl at any age, but are a little more common during adolescence.
The diagnosis protocol is to follow the hormones and their productions as outlined above. Treatment might be surgical or by hormonal injections and is best if initiated early because some things just can’t be undone.
The “Talk”
The process of puberty is far more unsettling and complicated than parents… well, probably any of us realize. The actual mechanics of generating and balancing and sequencing all the hormones and other components required to orchestrate puberty is at least as substantial as launching and building the space station.
The metamorphosis of a child’s entire physical being would be much more of a shock if it were instant rather than over 4 years; but, that’s what happens doesn’t it. If you hadn’t seen the child since she was seven you might pass right by her adolescent self if you met her on the street.
What I’m trying to say is: It’s a big deal! And it deserves much more than a passing, off-the-cuff “You good with the bees and bird stuff?” “Yep.” “Good. How ’bout them Kardasian’s?”
Parenting about puberty can begin at 5 or 6 in a nonchalant way, if the opportunity arises; but short and casual discussions about the pubertal body changes to anticipate should begin for sure by seven or eight.
Personally offering reading materials with an arrangement to explain/talk later may relieve some of the awkwardness. Notice I didn’t say just leave it somewhere where they will “accidentally” run across it on their own. Do you really want to leave launching the space shuttle to chance? And surreptitiously leaving books merely conveys loud and clear that you DON’T want to talk about it and it’s something that they should worry about discussing with you directly.
The follow-up discussions can then be short but recurring and informative but casual. You shouldn’t plan on getting through it all in one sitting; but it will then be clear that both you and the subject are approachable and geared toward helping them, for example: “avoid the mistakes and misunderstandings that I made.” That, after all, is the goal: no surprises and making it as easy as possible.
Hygiene
 Puberty talks can begin with hygiene
Puberty talks can begin with hygieneTalks about hygiene can begin even before puberty sets in and pave the way for open discussions about bodily functions.
Most of the changes that will occur during puberty for both boys and girls require greater care and attention than in their whole life up to this point. This means taking more time to clean their body, especially the genitals.
While children may get away with an every other day bath, adolescents should bathe every day: treating acne, using mouthwash and applying deodorant. Teens sweat more and the sweat contains different compounds which now give off odors. Odors which their own sense of smell “adapts” to easily causing them not to smell how smelly they are. Daily bathing, deodorants and antiperspirants “will have their backs.”
Girls will naturally have an inoffensive, slight sweetish smell from the vagina once puberty begins. If the odor is strong or foul it probably indicates an infection for which medical attention should be sought and treatment begun. The odor will resolve with the infection.
Vaginal discharge is a necessary part of the body’s regular functioning and normal discharge is usually clear to white as the body is self-cleaned. The discharge will sweep away bacteria which helps prevent vaginal infections. Parents should stress that girls clean the vaginal area with a mild soap and water – trying to wipe, just like after using the toilet, “front to back” in order to avoid contamination.
Still More to Come
Even after a child reaches Tanner stage 5, they are not done “maturing.” The Tanner scale does not include neurological functioning, in fact most of what we know now wasn’t even thought of back then.
Emotions and behavioral control functions don’t settle down or develop completely until, perhaps, 21 or so. And I have to say, in some parent-child situations, the physical changes can be the least of the difficulties.
We’ll discuss more about the pubertal changes unique to boys in the next post of the series and the emotional/psychological aspects in the post after that.
10 Posts in Puberty Talk (tanner) Series
- Boys Underwear: Boxers, Briefs or Commando - explanation, recommendations – 22 Sep 2018
- FAQ - Boxers, Brief's or Commando – 28 Aug 2018
- Doctor's Talking About Puberty and Sex to Patients – 28 Aug 2017
- Video: Puberty Time Lapse – 5 Jul 2017
- Puberty: Psychological Stages - Part 2 – 13 Aug 2015
- Puberty: Psychological Stages – 5 Aug 2015
- Tanner Stages - Boys – 28 Jul 2015
- Tanner & Growth - Girls – 20 Jul 2015
- Tanner Stages and Growth – 12 Jul 2015
- Puberty, Tanner Series: Intro/Index – 11 Jul 2015
Advertisement by Google
(sorry, only few pages have ads)