
Puberty: Tanner Stages – Boys
Boys and puberty – what a topic. We’re told that only two people in the history of planet earth got to skip puberty, so it’s obviously a phenomenon which has been afflicting earth children since … forever.
We’re still trying to figure it out, but the task was made much easier around 1948 when Dr. James M. Tanner, a British pediatric endocrinologist trained in the U.S., was asked to take over the “Harpenden Study” by the British Government.
A vintage photo of 10-year-old boys taken for the school health program
The study had been started during WWII at the Harpenden orphanage in order to study the effects of malnutrition on children. Remember, back then almost nothing specific and concrete was known about diet and nutrition except there was probably good and bad and you really needed to keep some foods cold.
Taking over the study was Tanner’s road to becoming the world’s leading authority on child growth and development. Trying to meticulously document all the orphans’ nutrition and growth status, he and his team fully examined each child bimonthly, taking measurements and photos and correlating them with their nutrition and treatment.
They did find that children’s growth could indeed be “stunted” by malnutrition; but could also be mostly made up for, if they were later treated kindly and nourished. Even more than that, he noticed other “standards” of normal growth and was able to design a chart describing five “stages” of puberty, whose “normal ranges” could be quantified for other physicians – prompting still further research and discoveries.
The only problem was that, even though progression through puberty could be well described, the “when it started” part was very, very, very variable.
For example: The pituitary sends signals to begin producing a boy’s puberty-inducing hormones (Stage 1) somewhere in the 4 years between 9 and 12. [In a girl those signals have their start anywhere along the 4 years between 8 and 11.]
Dr. Tanner and Puberty
 Puberty begins surreptitiously, often not soon enough to suit boys
Puberty begins surreptitiously, often not soon enough to suit boysObviously starting the hormones a-flowin’ comes before any actual body morphing is noticeable – which, again, takes another 1 to 2 years, extending the variability even further.
Why is there such a big range? Who knows! Genetics, nutrition and other environmental factors, activity levels, stress, additives and other adulterations in food – all of them are logical and are thought to have some possible undefined effect but nothing’s been proven.
The fact is that the differences between children seen in school classrooms for grades 1 – 4 seem nothing compared to classrooms full of 5th through 7th graders – which become very strange indeed. Some school districts even invented “middle school” to control the chaos.
Tanner wrote that: “90% of an individual child’s adult height is based on genetic factors, but the environment is the key factor when thousands of children are studied.” Then, after years of further experience, he concluded with the reprimand that: “community-wide data on adult height was an indicator of how a society fosters its youth!”
The Tanner scale then, is a: “scale of physical development in children, adolescents and adults, which defines physical measurements of development based on external primary and secondary sex characteristics; such as: the size of the breasts, genitalia, development of pubic and axillary hair and, for boys, testicular volume.”
Let’s take a look at the several stages a boy goes through during puberty.
Stages of Puberty in Boys
- Stage One (approximately between the ages of 9 and 12) — the “maturifying” of boys, as it does in girls, begins surreptitiously when the hypothalamus in the brain sends a “signal” to the Pituitary (also in the brain) that it should begin orchestrating the complex hormonal process which will change this boy into a man.
The hormones begin flowing, but no outward physical changes are usually noted; although, if one wanted to obtain blood samples, the surge in hormones could be measured. Growth rate is usually no greater than it has been through childhood. Erections, which in the first couple of months of life were frequent due to maternal hormones, are still infrequent.
- Stage Two (approximately between 9 and 14) — Stage two is probably what most boys, parents and physicians are watching for and gets the most attention. Of hair, voice, skin and genital changes, the growth of the gonads is the easiest and most consistent sign that puberty has started and the growth spurt is beginning. Once you can say stage two has begun (testicle length 2.5 cm), muscle tissue and fat begin to increase. The face starts to change in appearance, blemishes begin to occur, and attitudes start to “morph.”
Actual growth in height starts quite slowly in stage two but increases velocity toward the end. A small amount of thin, light pubic hair begins at the base of the penis. Testicles and scrotum grow but the penis probably does not. Erections are becoming more frequent. The aureole, the dark skin around the nipple, darkens and increases in size – yes, even in boys.
- Stage Three (approximately between 11 and 16) — This is the stage when the penis begins to grow, in length rather than width. Pubic hair is darkening, becoming a little more coarse and spreading toward the groin from the pubis. Testosterone has reached the level where erections are frequent and noticeable and can be ill-timed, occurring seemingly without provocation.
Appetite has increased even more as height growth velocity is reaching its peak – even slightly obese children often look like they are thinning out; and faces are changing, dramatically in some children. Shoulders broaden, facial hair grows on upper lip and voice “cracks” as the voice-box begins to protrude in the neck and voice deepens. Breasts have darkened and may show some protrusion due to normal hormonal growth (gynecomastia) – yes in boys too.
- Stage Four (approximately from 11 to 17) — The growth spurt in height is already well underway and now the genitals darken, become rugated and the penis grows in width as well as length.
Underarm and facial hair increase, become thicker and hair may begin to grow around the anus and on the chest, arms and legs. The skin gets oilier and the voice continues to deepen.
- Stage Five (approximately between 14 and 18) — Stage five is when the adolescent takes on the physically adult appearance. Adults are considered stage five the rest of their lives. Height velocity has slowed considerably now and will eventually cease altogether when the bone growth-plates fuse (rarely as late as 21). Based on ethnicity the hair will reach its greatest extent and shaving is a necessity; and the voice has changed to the tone and timbre it’s destined to be.
Genitals are adult male and erections are at adult levels and more controlled. Sweat glands have developed and acne has usually subsided. Any breast tissue development (male gynecomastia) has resolved or is much less prominent under the enlarged pectoral musculature. Much of the emotional rollercoaster-drama has subsided or will in the next couple of years [although parents may not become ‘smarter’ until their early ’20’s (the boy’s, not the parents). The boy has become a physical ‘man’; however, just like stage five girls, he is not emotionally/psychologically mature. (More on that in the last post of the series)
Summary of Physical Findings
| Stage | Genitals | Testicle length | Pubic hair | Height velocity/yr | Other |
|---|---|---|---|---|---|
| I | Infrequent erections | Less than 1.6 cm (5/8 in) |
Villus hair only (through age 11 years) |
5.0 to 6.0 cm (2 to 2-1/2 in) | Prepubertal: no sexual development, Adrenarche |
| II | Scrotum skin thins and reddens, Frequent erections | 2.5 to 3.2 cm (1 to 1-1/4 in) |
Sparse, slightly pigmented (average 12-1/2 years) |
7.0 to 8.0 cm (2-3/4 to 3-1/4nbsp;in) |
Testes enlarge, Body odor, Leaner body |
| III | Lengthening of penis | 3.3 to 4.0 cm (1-3/8 to 1-1/2 in) |
Coarser, darker, curled (average age 14 years) |
8.0 cm (3-1/4 in) |
Pubic hair starts growing, Ejaculation (wet dreams), Temporary swelling of breasts, Voice breaks |
| IV | Thickening, darkening of penis and scrotal skin | 4.1 to 4.5 cm (1-5/8 to 1-3/4 in) |
Adult type, but not beyond pubic area (average age 15 years) |
10.0 cm (4 in) | Pubic hair curlier and coarser, Height spurt, Male breast development, Acne, Underarm hair, Voice deepens |
| V | Adult genitals | 4.5 cm (1-3/4 in) |
Adult type, spreading onto inner thigh (average 15-1/2 years) |
Full height reached at age 18 or 19 | Fully mature male, Pubic hair extends to inner thighs, Increases in height slow, then stop, Beard, Continuing muscle dev. |
Issues in Puberty
Most of the time issues with puberty have to do with things being either “too early” or “too late.” Since the time when Dr. Tanner did his work, there is some logic now in the decision to begin the hormone workup necessary to diagnose development problems and not just be pushed by wishes and perceptions.
Diagnosing both delayed and premature puberty requires measuring several hormones in order to determine which are lacking or which are in excess. There are blood tests for each one, but they are a bit expensive and “being normal” is a diagnosis of exclusion after all of them are completed. Therefore, it’s nice to actually have an index of suspicion that things aren’t normal before you start the expensive workup.
If a tumor is suspected, imaging of the suspect organ needs to be done as well, with x rays, computed tomography scans (CT scans) or magnetic resonance imaging (MRI).
And lastly, the mere “definition” of both sexual precocity and delay seem to be moving targets. We know that “normal” puberty is beginning earlier and earlier, so our “cutoff age” for abnormal is being revised lower too – thought to be related to better (or excessive) nutrition.
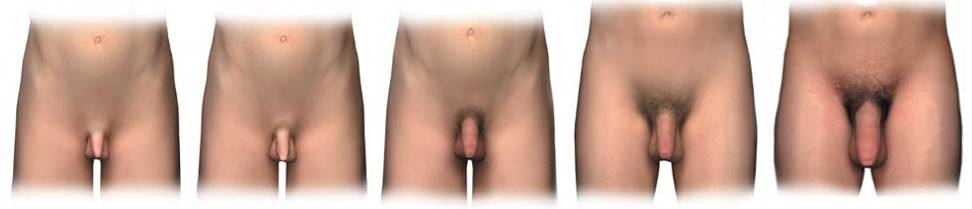 The five Tanner stages of puberty in boys
The five Tanner stages of puberty in boysTiming: Premature Onset
In these modern, industrial times breast development before age eight or first menses prior to ten are the newly established lower limits for early puberty in females, and any changes in a boy prior to his ninth birthday would be worth noting – and perhaps working up with at least a thorough physical exam and possibly blood work and wrist x-rays to calculate a “bone age.”
Bone age is normally about 18 to 24 months behind the chronological age; and with the use of tables, allows us to estimate how long the growth plates still have before they close off. That will show how much growth there still will be. The earliest triggers of puberty usually start by the time the bone age reaches 12 years of age in boys.
Symptoms of precocious puberty in boys are those of normal puberty, just earlier: the development of a large penis and testicles, with spontaneous erections and the production of sperm. Also hair growing on the face, under arms and in the pubic area, and acne.
Excess hormone production might be coming from anywhere along the complicated line of glands from the brain to the gonads and adrenals or other places via tumors. Brain overproduction of hormones might also be the result of brain infections or injury.
Timing: Delayed Onset
Our definition of “delay” in puberty is a bit in question these days too. Because the “earliest date” is getting lower and lower, should we also then be reducing the expected “late date” by that much as well? Some of us do, but some don’t.
The penis and testicles not enlarging, easily noted on a physical exam if one is done, before the fourteenth birthday in boys is generally accepted as a cutoff point to begin considering a further medical investigation. But some of us modify that by also delving into where the child stands now on the growth chart, where he’s stood in the past, parent’s and siblings heights and other family member’s experience with puberty.
It might sometimes be justified to begin a “delayed puberty” workup at 13 in boys. Because it is easy to determine the size of the testicles on a physical exam, having very small testicles or testicles that cannot be readily felt is a clue to the condition. There are several causes, including: previous surgery for undescended testicles or cancer treatments, which can injure the testicles; several different endocrine and metabolic diseases; environmental/nutritional conditions; medications; and, strenuous exercise.
 Delayed or precocious puberty can be stressful, more-so in boys
Delayed or precocious puberty can be stressful, more-so in boysIf the penis is small but the testicles have begun to grow, other signs of puberty should appear in the next 6-12 months. Boy’s growth spurts don’t occur as early in the puberty process as the girls do.
What you must remember is that even though boys with “constitutional delayed puberty” (i.e. family trait) might be short when compared with their current peers, they nearly always catch up to them by the time they are 18 – and have heights in the normal range as adults.
That being said, on occasion where there is bullying or other stress factors, and even though it’s not without risk, a pediatrician may elect to offer a brief course of testosterone after age thirteen that might “jump-start” puberty.
A monthly injection for several months (different doctors use different doses and frequency) until early genital changes and growth in height has occurred may be all it takes to then let the body take over on its own. The limited studies done so far don’t seem to be indicating early growth plate closure and loss of adult height with the technique; but the jury is still out.
Additionally, there are medications (like those for ADHD) which can cause loss of growth. During the times where puberty is expected, weight loss due to those drugs can be masked by merely assuming a “normal constitutional delay.” It becomes very important to follow growth and Tanner staging in order to be able to decide whether or not to stop those medications.
[AAP: Delayed Puberty https://www.healthychildren.org/English/ages-stages/gradeschool/puberty/Pages/Delayed-Puberty.aspx]
Abnormal Hormone Production
Just as girls might have “virilizing syndromes,” in boys there can be estrogen producing tumors. The effects are a bit different in that there is usually also enough testosterone secreted to initiate male puberty changes as well.
Remember, from your high school genetics course, virilizing requires abnormal male hormones in the female. Every embryo’s base state is female-like then genetically controlled male hormones develop it into a male. Therefore, later in life, estrogens in a boy don’t “take away” the maleness that is already there, they usually just cause abnormal breast development.
The “Talk”
The process of puberty is far more unsettling and complicated than parents… well, probably any of us, realize. The actual mechanics of generating and balancing and sequencing all the hormones and other components required to orchestrate puberty is at least as substantial as launching and building the space station.
The metamorphosis of a child’s entire physical being would be much more of a shock if it were instant rather than over 6 or so years (in boys); but, that’s what happens doesn’t it? If you hadn’t seen the child since he was eight you probably would pass right by his adolescent self if you met him on the street.
What I’m trying to say is: It’s a big deal! And it deserves much more than a passing, off-the-cuff “You good with the bees and bird stuff?” “Yep.” “Good. Good, good… How ’bout them Mets.”
Parenting about puberty can begin at 5, 6 or 7 in a nonchalant way if the opportunity arises; but short and casual discussions, about the pubertal body changes they can anticipate, should begin for sure by seven or eight.
 The “talks” about puberty should begin by age 7 or 8
The “talks” about puberty should begin by age 7 or 8Personally offering reading materials, with an arrangement to explain/talk later, may relieve some awkwardness. Notice I didn’t say just leave it out somewhere where they will “accidentally” run across it on their own. Do you really want to leave launching the space shuttle to chance? And surreptitiously leaving out books or pamphlets, merely conveys loud and clear that you DON’T want to talk about it and it’s something that they should be afraid of discussing with you directly.
The follow-up discussions can then be short but recurring, and informative but casual. You shouldn’t plan on getting through it all in one sitting. It will then be clear that both you and the subject are approachable and geared toward helping him, for example, “avoid the mistakes and misunderstandings that I made.” That, after all, is the goal: no surprises and making it as easy as possible.
Hygiene
Talks about hygiene can begin even before puberty sets in and can pave the way for open discussions about bodily functions.
Most of the changes which will occur during puberty, for both boys and girls, require greater care and attention than they’ve given it during their whole life up to this point. This means taking more time to clean their body, especially the genitals.
While children may get away with an every other day bath, adolescents should bathe every day; treating acne, using mouthwash and applying deodorant. Teens sweat more and the sweat contains different compounds which now give off odors. Odors, which their own sense of smell “adapts” to easily, causing them not to smell how smelly they really are. Daily bathing, deodorants and antiperspirants “will have their backs.”
Boys, who are stereotypically much more in love with “puppy dog tails” and eschew bathing of any sort, might be especially inclined to be “too busy to wash” and need extra attention in this area.
They should be instructed to wash their genitals every day. This includes washing the penis, the scrotum which holds the testicles, the anus, and pubic hair, with water and mild soap.
Uncircumcised boys need to be instructed that the foreskin should be pulled back daily to expose the tip of the penis, which should also then be washed with mild soap and water.
Still More to Come
Even after a child reaches Tanner stage five they are not done “maturing.” The Tanner scale does not include neurological functioning, if fact most of what we know now wasn’t even thought of back then.
Emotions and behavioral control functions don’t settle down or develop completely until, perhaps, 21 or so. And I have to say, in some parent-child situations, the physical changes they’ve gone through can be the least of the difficulties.
We’ll discuss more about the emotional/psychological aspects in the next posts of the series.
[Child Development Institute. http://www.childdevelopmentinfo.com]
10 Posts in Puberty Talk (tanner) Series
- Boys Underwear: Boxers, Briefs or Commando - explanation, recommendations – 22 Sep 2018
- FAQ - Boxers, Brief's or Commando – 28 Aug 2018
- Doctor's Talking About Puberty and Sex to Patients – 28 Aug 2017
- Video: Puberty Time Lapse – 5 Jul 2017
- Puberty: Psychological Stages - Part 2 – 13 Aug 2015
- Puberty: Psychological Stages – 5 Aug 2015
- Tanner Stages - Boys – 28 Jul 2015
- Tanner & Growth - Girls – 20 Jul 2015
- Tanner Stages and Growth – 12 Jul 2015
- Puberty, Tanner Series: Intro/Index – 11 Jul 2015
Advertisement by Google
(sorry, only few pages have ads)