
Hyperactivity Treatment: Cognitive Training, Medication or Both

I’ve explained about how prevalent and confusing the “placebo effect” has made this whole subject and given you a list of the many, many so-called “secret treatments” which have been proven to be no more than a waste of money. And you’ve learned that there are only TWO treatments which have been proven to be effective: Cognitive therapy and medication.
Causes of ADHD
Clues To Causes and Contributors
Causes
Literally hundreds of thousands of research studies have been done on various aspects of ADHD. That’s partially because science and medicine has known something was up and been wondering about it for probably hundreds of years.
Symptoms of forgetfulness, distractibility and hyperactivity levels (just like we see in ADHD) were seen to occur even in ancient times after many types of “insults” to the brains of people. Total changes in personality and actions.
Closer inspection, records and experience looking for those traits showed many people also were born with them; and just lately statistics are good enough to estimate the “mean heritability” of ADHD at 76%—making it one of the most heritable “psychiatric” disorders.
Strangely, ADHD is three to five TIMES more common in boys than in girls; and girls have much more of the “predominantly inattentive” type while boys have the “hyperactive type.”
The hundreds of thousands of studies are due largely to people trying to “prove” some pet (usually lucrative) hunch they’ve got about causes or treatment which have NOT proven true. But it HAS left us proof that “DIET, ESPECIALLY SUGAR, IS NOT a cause of ADHD” even though we still don’t know what is.
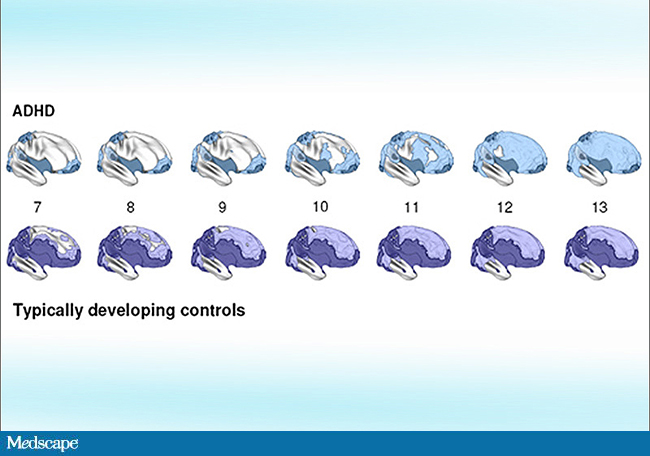
The graphic is a composite of what studies have found using new MRIs in both children with ADHD diagnosis and those without it. It shows cortical thickness which normally thickens with age. It seems the “thickening” (darkness) is delayed in ADHD.
Further, expensive PET scans have now been done on some people with ADHD and found lower dopamine activity in the limbic system, but not in all. That explains why medications which increase dopamine are effective in treating ADHD (methylphenidate).
Such scans also show evidence of “frontostriatal” malfunctioning and deformations in the basal ganglia which actually become “normalized” when ADHD patients use stimulant medications. Other research shows a “dysregulation” of the neurotransmitter norepinephrine associated with ADHD.
For some of us it’s maddening to see how close we’re getting to understanding this better but still can’t quite get a definitive answer. Personally, I’m disappointed we’ve wasted so much time needing to disprove schemes instead of focusing on things that matter.
Contributors

The role of family environment in ADHD is unclear but it certainly may exacerbate symptoms and/or alter the effectiveness of treatment. And we now know that ADHD is associated with other clinical diagnoses as well—antisocial personality disorder, self-injurious behaviors and addictive behaviors (unrelated to ADHD medicine).
Additionally, even though they are not causes, environmental and sociological factors shouldn’t be left out of the discussion. Stress, conflicts, pressure, family dysfunction and the mere phenomenon of being labeled with ADHD may exacerbate a child’s current symptoms of ADHD and even produce other symptoms not initially present.
So, let’s spend the remainder of our time together talking about the two things we KNOW will help your son or daughter who happens to have ADHD, even before we fully understand why, so that things which CAN be done ARE done while they still can be.
“Cognitive” training (i.e. counseling and therapy)—because insight, reasoning, knowledge and training are the only things which produce truly long-term beneficial changes of behavior; and, medicines—because that’s where the TRUE science as well as experience tells us the real help presently comes from.
Effective Treatments
Only True Hope For Improvement – “Best Taken Together”
Medication
Out of habit I think to write about cognitive therapy first because it’s so often overlooked. However, the child’s response to a trial of medication is so critically important, most of us don’t even think we’ve got the diagnosis until it’s complete—we should talk about it first.
Frankly, if the situation doesn’t allow me to have a child’s parents obtain three consecutive, weekly questionnaires from an UNKNOWING spouse and teacher, while the knowing spouse gives the child a trial of medication only one of those weeks—well, I just get an uneasy feeling in my gut that we might be missing something.
It is the most common of things to have a teacher call a child’s parent and ask “what’s happened with Johnny? Today’s been GREAT!”—on the very day the surreptitious trial of medicine has begun.
The results are often so dramatic it’s hard to keep the trial “blinded” to anyone who regularly spends time with the child, they just “know” something is up. NOT sleepy, NOT tired, NOT “spacy”—just less Distractible, more attentive, less impulsively disobedient and disruptive. Homework and projects are actually done, concepts understood, friends not alienated!
The effects and role of medication in ADHD has been studied extensively. Clear back in 1999 a massive study was done by the National Institute of Mental Health following children with ADHD for over a full year using the only four treatments which showed consistent help: three similar forms of counseling and medication.
In the study, teachers, parents and other care-givers did extensive evaluations and medication accounted for the largest improvement in ADHD symptoms. The addition of behavior treatments resulted in additional gains which normalized behavior.
Findings of well over 150 controlled, double-blind studies of medication in ADHD, consistently and extremely well document that children improve attention span, self-control, behavior, fine motor control and social functioning.

Today, in 2017, we have two classes of medication: methylphenidate and amphetamine related products. There are short acting and long acting types, so children no longer need to rely on “the kindness of teachers and nurses” to receive their medications.
The best thing to do is discuss medication options with your doctor because each product has slightly different action times and side-effect profile which should be tailored to a specific child’s diagnosis, situation and response.
Just be aware that the new medicine Atomoxetine (brand name Strattera, heavily marketed by the company using “scare tactics” touting it is “non-stimulant”) needs to be taken in the proper perspective. It has been shown to work in some ADHD; but, it does so by acting on the noradrenergic system (instead of the adrenergic system), is a LOT LESS studied, still has its own side-effects and may not even produce results for up to three weeks.
Therefore, no one should use Atomoxetine for a diagnostic trial like I’ve mentioned. There are times where it might be indicated, such as when ADHD is associated with depression; and sometimes even other medicines may be added (like Clonidine and Tenex) for specific children, like those who are very hyperactive and/or impulsive.
What I’m saying is that each child deserves to have their ADHD treatment individualized specifically to them. AND, they need to have a doctor who not only takes the time to be certain of the diagnosis, work with the teacher and school but has a plan to follow-up and coordinate all aspects of treatment.
Nearly all known side-effects of medication resolve on their own with time or are soon adapted to in some way. However, sometimes a change to a different medication is needed. How will you ever know that, if you don’t follow the patient closely? Make sure children get a good physical exam at least yearly within all their followup visits, and for some more often.
Cognitive Training
The single other treatment option that works for ADHD is “cognitive training”—which most of us just call “counseling” because that is the setting in which it is often received. It is where the abundance of “actions” produced by the ADHD are turned into the “chosen behaviors” more appropriate for success in society.

Unless you have ADHD yourself (and therefore “watched” your own parents do their “parenting” on you) you have probably never been taught how to “parent” an ADHD child. SO, not only does your child who is being diagnosed with ADHD need Cognitive Training; you need training on how to perform it yourself.
In fact, if your child’s doctor want’s to begin medication for ADHD and hasn’t also suggested “counseling” then ask for it! If the counselor you are referred to spends all the time with the child and doesn’t teach you skills; then either ask them for it yourself or ask for a referral to someone else.
Yes, it’s that important! I never merely just expect or assume any parent to already know how to parent a child with ADHD. It’s not the same, and not an inborn skill, especially this day and age.
Almost always (once a correct diagnosis is made) when a parent tells me the medicine isn’t working I find it’s because they are expecting the pill to “teach” them how to behave.
It does not. Medication DOES DO what I’ve listed above to lessen the amount of inattentive/impulsive behavior; BUT where do they “learn” what behavior is appropriate? That’s what counseling and parenting does for a child and each child is different.
The fancy word for what most parents and teachers do to most children is: Cognitive-Behavioral Interventions. That is basically teaching problem-solving skills and self-control through report cards, star-charts, rewards and the normal coercions of parenting. However, there is an “absence of strong research to support its efficacy [in ADHD]”; which, is why we’re talking about this in the first place.
The Cognitive Training that works comes in basically three intensities: Clinical Behavior Therapy (CBT), Contingency Management (CM) and Intensive Behavioral Treatments. The latter two are basically more intensive kinds of the first one done in facility or “in-patient”/residential settings.

The stated goal of Clinical Behavior Therapy is: “to train parents, teachers or other caregivers to implement contingency management programs with children.” Huh?!
What this means in “normal speak” is that tokens, points and report cards are still used but on a daily, more timely basis.
Parents also learn how to: identify inappropriate behavior worth changing, “reprove betimes with clarity” and not belittlement, reward positive behavior, problem-solve for appropriate behaviors to use instead and have them practice it until learned.
This obviously is more time consuming and difficult than merely taking a pill. It’s, of course, what those who succumb to the false rhetoric and fear published on the internet need to do if they want to “treat ADHD without pills” like their titles proclaim.
Combination Therapy
Most intelligent people can see what a self-defeating catch-22 this can be: pills don’t teach specific behaviors but counseling does, counseling can’t be effectively learned because the ADHD symptoms are still there without the pills. Talk about a vicious circle!
A song popular in my age proclaims “you can’t have one without the other.” In this case, you can have them alone; but WHY WOULD YOU unless symptoms are minor or other coping mechanisms are already in place? The two together, in most instances, make the child “whole” or equivalent to their age-mates and give them a better chance in life than either one alone.
Once treatment is underway, using the combined approach may allow either one or the other or both to be scaled down. When a good component of behavioral treatment is being used, the dose of medication can often be reduced and the “back-sliding” is much less when any medicine hiatus is given; such as perhaps in summers, on vacations or other accidental times.
Conversely, the behavioral component, the most time consuming and “draining” aspect for parents, is much less often required during the day and definitely easier and more effective when medication is effectively used. And, the need for “time-outs” and “talk” sessions are less frequent and rewards can be given more often.

A child identified by the school system already has a leg up on treatment because several laws mandate it. Parents can capitalize on it because most schools I’ve ever connected with are MORE than happy to have parents involved and their counselors are MORE than willing to teach.
Physicians should capitalize on it as well, schools are a tremendous resource for skilled experience and help as well as an UNBIASED source of information, diagnostic and otherwise. The only motive they have is to see that the child gets educated.
☤
The goal of writing this series was not to diagnose a specific child, nor to espouse one treatment over the other; only to provide a common sense source of actual research and experience for how things can be handled in the best way.
Hopefully, it can help you navigate through the system and give you some standard to compare whether the care you are receiving is on track to the best outcome.
13 Posts in ADHD Hyperactivity (hyperactivity) Series
- Hyperactivity & Puberty - Part 2, Issues and Actions – 22 Jan 2019
- Hyperactivity & Puberty - Part 1 – 10 Jan 2019
- The Children - Followup and Outcomes – 26 Mar 2017
- (Link) Don't JUST take my word for it – 23 Feb 2017
- Treatment: Cognitive Training, Medication – 18 Feb 2017
- Treatment: Five Pillars of ADHD Treatment – 4 Feb 2017
- Treatment: How can we know what works? – 29 Jan 2017
- (Video) Sucess in 'Something' Helps – 20 Jan 2017
- The Patient – 15 Jan 2017
- First, the diagnosis – 11 Jan 2017
- Labels and 'Alphabet Soup' – 7 Jan 2017
- Treatments - 'alternative' – 6 Feb 2013
- ADHD Hyperactivity: Intro/Index – 5 Feb 2013