
3 Rashes And Their Heart Problems

We’ve chatted about rashes before (ok, a lot) and we’ve talked about heart diseases before. Heart diseases only very rarely are associated with rashes. And only an infinitesimally small number of rashes cause heart disease. When they do, it’s worth talking about… so let’s chat about rashes and heart.
A boy with acute rheumatic fever undergoing an echocardiogram
A tiny disclaimer to begin: I’m not going to give an exhaustive list of all rashes and all heart diseases only three of them. Fortunately, the combination is fairly rare in childhood. AND, remember it’s NOT the rash that’s causing the heart problem, it’s “something” that causes both together in association.
These three rash/heart-problems are the most common although I bet you there are substantial numbers of doctors who are making it all the way through medical school these days without witnessing a single patient with the first disease on the list: Acute Rheumatic Fever.
Rashes and Heart Disease in Children
Acute Rheumatic Fever, ARF as it is called, was once a terribly common disease on the tips of most parents tongues. We all lived in fear of strep throats turning into ARF – even substantially long after the cause and treatment of the problem was discovered.
Erythema Marginatum and ARF

Penicillin cured most of the strep organisms which were causing ARF BUT it needed to be taken early enough and long enough to prevent the body itself from making the antibodies against the bug; which would then turn around and also attack the persons heart.
It took a long time to convince parents of that fact, and still today unknowing people stop their 10-day-course of antibiotics after only a couple days when the sore throat seems healed. Not good. Finish all your medicines just as the doctor prescribes!
Because sore throats (and other infections) are caused by a particular kind of bacteria, a child may have recurring “attacks” of ARF.
A rash known as Erythema Marginatum (sometimes as erythema annulare) may occur along with the infection – usually at the beginning, more often with the first episode of ARF and sometimes with other signs too.
In the first episode about 10% of children developed the rash, overall about 5% do. Subcutaneous nodules (firm bumps just under the skin) are thankfully also rare in ARF but when they do occur it is usually with inflammation of the heart as well, many weeks after the onset of the disease.
Erythema Marginatum is a pinkish, mostly flat (occasionally slightly raised), non-itchy, short-lived rash. Usually on the trunk and upper arms and legs. Nodules, if they occur are painless and mostly over bony prominences.
The heart inflammation of ARF is what we call a “pancarditis.” “Carditis” because it is an inflammation (“itis”) of the “cardium” or heart and “pan” because it effects most aspects of the heart: pericardium, epicardium, myocardium, and endocardium.
Other associated side-effects, which help physicians make the diagnosis, are the involuntary writhing of limbs known as Chorea (Sydenham’s chorea, or St. Vitus Dance) and the hot, red, migrating arthritis of large joints
Good pediatricians and pediatric nurses don’t take infections with “strep” lightly, neither should you. Obtain appropriate throat cultures and “strep” tests and take ALL your medicines in a timely manner.
Kawasaki Disease and strawberry tongue

In my medical school days we learned about Kawasaki Disease but thought of it as mostly a “Japanese disease” – because that’s where nearly all of the cases were being found at the time and was where the disease was characterized. A case of it coming to our hospital was definitely a “grand rounds” presentation case.
That’s no longer the case however, and it’s quite common in “the states.” There are even several competing “official” web sites in “support” of those with the disease.
Kawasaki’s Disease, or KD as it is known on the internet, has two phases: the first where the high, unrelenting fever makes life miserable, parents panic and doctors run a lot of tests; and the second where fever subsides but all kinds of major symptoms, including death, begin.
ACUTE PHASE
KD is basically a febrile vasculitis syndrome of early childhood.

It’s the fairly high, unrelenting fever that usually brings the child to the attention of the doctor. The fever may slightly respond to fever-medicine or not, but it lasts for 3 to 5 days, quite unusual as acute illnesses go.
Just before the fever breaks (or at the same time) the inflammation of the body’s blood vessels cause redness in both eyes (conjunctivitis – 90%), a deeper eye infection (uveitis – 70%) with blurred vision, redness around the anus (perianal erythema – 70%), and redness and swelling of the lips, tongue, hands and feet (erythema and edema).
SUBACUTE PHASE
The fever does eventually subside and occasionally it’s not until this phase that the diagnosis is finally made. KD often causes the skin on the digits to peel off (desquamation) AND it is now that the results of the previous several days of infection shows up in the heart.
During this phase, a coronary aneurysm may develop and the risk of sudden death is highest.
KD causes not only weakening of areas in the blood vessels but blood-clotting-cells (platelets) increase and risk causing a clot.
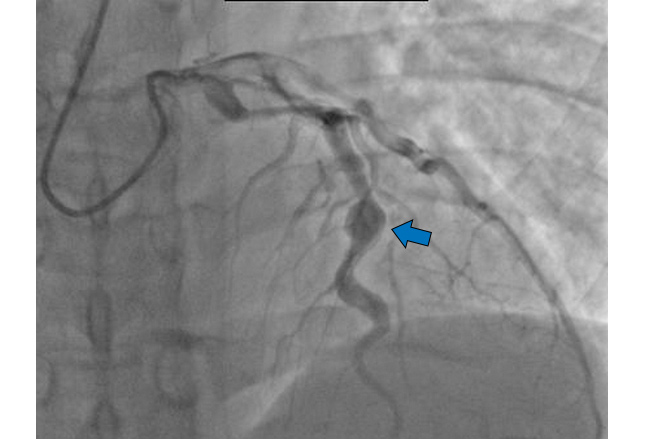
Prompt treatment with intravenous immunoglobulin (IVIG) and high-dose aspirin is the current standard of care. Coronary aneurysms (shown) occur in 25% of patients not treated with IVIG, compared with approximately 1-5% of patients treated with it.
Aspirin has a synergistic effect with IVIG, so it is initiated at a high dose. Aspirin may be continued at a lower dose for its antiplatelet effects to further reduce the risk of thrombus formation.
Bacterial Endocarditis and Splinter Hemorrhages

Of the three conditions I’ve listed here, Bacterial Endocarditis and their ‘splinter hemorrhages’ must be the least common in children.
Endocarditis is when an infection attacks the lining of the heart or endocardium. As I’m sure you can assume, it’s not a good thing because little ‘bits’ of infected material are then in a prime place to get carried in the blood to other parts of the body where they can lodge and cause problems there too.
Why would the lining of the heart become infected? Well, it’s usually because there’s some abnormality in the tissue that weakens the area and allows infection to begin. But there are other possibilities too so diagnosing endocarditis is often just the first dilemma for a doctor.

In younger people the bacteria is often one of the kinds of Staphylococcus which are the ones that causes skin infections too – and the kind that may have learned how to defeat all our antibiotics.
In a young patient with presumably normal heart valves, acute onset of fever and chills, heart murmur, and Janeway lesions (shown) infective endocarditis is the most likely diagnosis.
Other cutaneous manifestations of infective endocarditis include splinter/subungual hemorrhages (arrow).
Acute endocarditis, in particular, requires prompt diagnosis and treatment, because its mortality rate is as high as 50%.
There are a few other combinations of heart issues and rashes seen together, Lyme Disease and Neonatal Lupus come to mind off the top of my head, but the three I’ve listed here are much the more commonly seen.
If nothing else, I hope that by reading this you get an understanding of why good pediatricians check for rashes and listen to the heart of about every kid we see!
Advertisement by Google
(sorry, only few pages have ads)