
Puberty: Tanner Stages and Growth

Pretty much the second question you field from a parent during your pediatric clerkship in medical school (right after “what’s this yukky looking rash”) is: “Do you think (insert name here) is growing well enough?” or, some equivalent question.
Doctor and Professor James Mourilyan Tanner (1920-2010), originator of scales to measure growth and development of children – pediatrician, endocrinologist
The clerkships are taken in your 4th year, before graduation, so you learn early to reply quickly “Well let’s see, it could be lots of things. Let me finish the exam and we can talk about it.” At least at my school, the attending would usually walk in before you were done so you’d have backup if by then you still didn’t have the answer.
The Tanner Scale
In the case of growth and development however, we had been completely and fully primed with an understanding of the topic – from infancy right through puberty and on to adulthood – largely thanks to “Dr. Tanner” the “inventor” of the “Tanner Scale.”
James Mourilyan Tanner
“The Tanner Scale,” well that’s what we call it now. Being a very non-presumptuous man, he would have never sought the limelight like that – he was an English gentleman after all, of the old school. He was a top-ranked hurdler (jumping hurdles) destined for the London Summer Olympics, except they were cancelled due to the outbreak of WWII. With his father in the British Army, and after his only brother was killed in the war, he decided to study medicine and was funded, by the Rockefeller Foundation, to study at the University of Pennsylvania with a small group of other UK students.
In 1948, after he interned at Johns Hopkins Hospital in Baltimore Maryland, the British government asked him to take over the “Harpenden” study of the children at the Harpenden Orphanage, which had been started in order to research the effects of malnutrition. In addition to histories of previous treatment and careful monitoring of their new nutrition, the children were simply and carefully measured and photographed every three months for analysis, in addition to receiving the latest in medical care.
Please keep in mind that, even at that time, next to nothing was known about normal growth and development of children, let alone any stages of puberty or maturation – things that every 6th grader is taught in school today. And even less was known about malnutrition in children and whether or not they were recoverable with treatment.
It was only through Tanner’s study that we now know that a child’s chronological age has only an arm’s length relation to their physical maturity level.
Tanner discovered and reported that “90% of an individual child’s adult height is based on genetic factors; however, when those characteristics are looked at across an entire society, they are a reflection of nutritional status and the care given to the society’s children.”
He did a whole lot more in his career too, like the initial work in the use of Human Growth Hormone. He became the world’s leading authority on children’s growth and development and stimulated many other physicians to dovetail and expand on his work. for example, similar scales were developed for x-rays: “Bone Age Scales”. They allow radiologists to look at x-rays and tell how mature the skeleton is compared to chronological age.
We’ve found that it’s a child’s “bone age” which correlates more closely to the “Tanner Scale” or “tanner stages” than the chronological age; and that is what allows us to answer another frequent question of parents: “how tall will he/she be?”
Tanner Scales of Growth and Development in Children
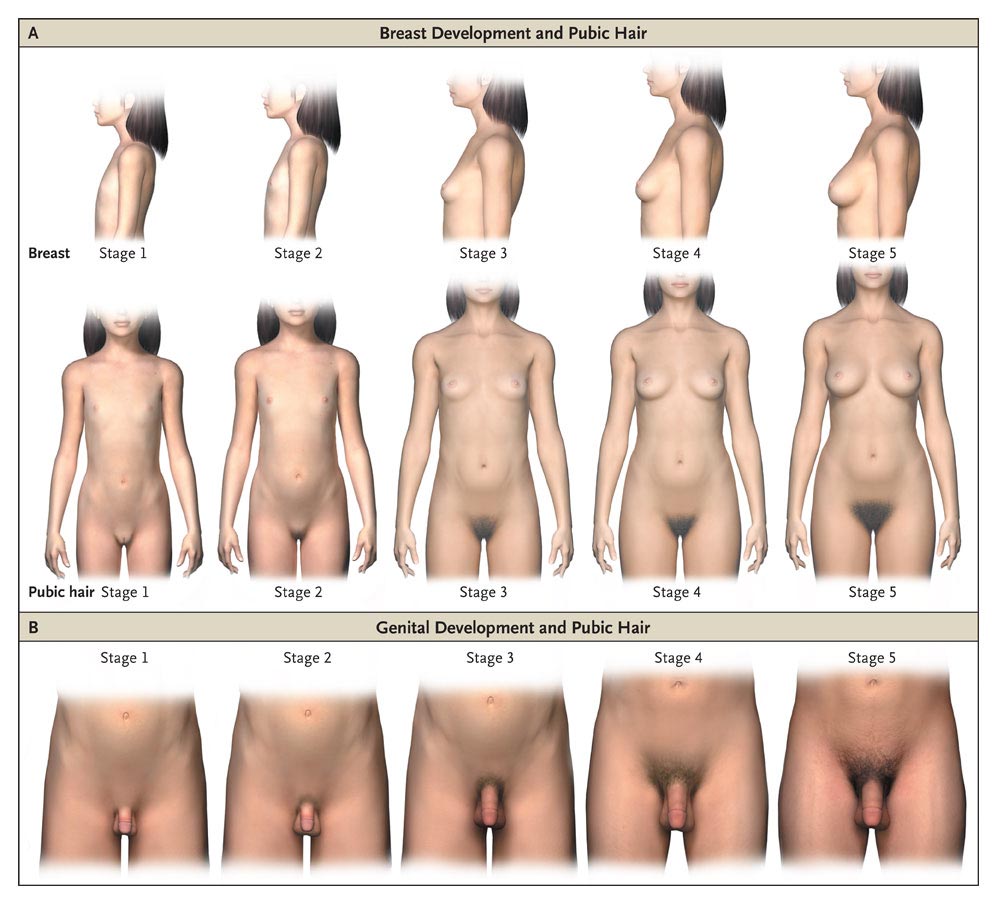 Graphic of Tanner Growth Scales showing 5 stages through puberty
Graphic of Tanner Growth Scales showing 5 stages through pubertyIt was Tanner’s careful measurements and photographs of the same children over 23 years, as they grew and developed through puberty into adults, which enables us to answer questions about growth in children today; and, to understand where and when a child begins to show signs of deviating from expected paths therefore needing further diagnosis and intervention.
Before the Tanner Scales, now used around the world, hidden endocrine problems usually weren’t identified until much too late to do anything about them. Some medicines we use today (for example the stimulants in ADHD) can sometimes interfere with growth and we use the Tanner scales to keep that from happening.
Whole treatment regimens for some diseases, like in AIDS, are modified based on maturity signals identified in Tanner’s research; because, not only do we want to avoid damaging growth, but the body reacts to drugs a whole lot differently as it stages through puberty into adulthood.
Tanner discovered that even though a child’s chronological age only vaguely related to the child’s maturity level, the progress of children through puberty did follow a pattern once it had begun. And he found that there were characteristic physical signs which could be measured to quantify their progression through those stages, such as size of genitals, breasts and pubic hair – the Tanner stages.
Height Prediction
Let’s take a hypothetical patient and answer the question: “How tall will he be?” [It seems to be mostly “he’s” that are asked about]
The standard, off the cuff, answer would be to reply: “A little more than half-way between your mother’s and father’s height.” The mathematical formula would be: [Mother’s height (cm) + 13cm + Father’s height (cm)] ÷ 2
So, if mom is 157 cm (61.8 in, 5.2 ft) and dad is 176cm (69.3 in, 5.8 ft) the child will be: 173 cm (68.1 cm, 5.7 ft), i.e. [157 + 13 + 176] ÷ 2. That is: IF the child’s puberty comes at the “normal” time – and sometimes that’s a big if!
You see most of the height is in the long bones, the legs; and all of the leg’s length is due to growth at the “growth plates,” the active cells at the ends of the bones. They are always growing a little through early life, until they close off as puberty ends, after which no further growth occurs.
Puberty hormones kick those growth plate cells into high gear for a while but eventually then cause them to close off. That is why actual height projection must be adjusted according to when puberty occurs; hence, the Tanner Scale. Early puberty causes a rapid growth spurt that ends prematurely, thus causing shorter height in adulthood.
 More than skin and bones mature in puberty
More than skin and bones mature in pubertyIf a child’s growth spurt and puberty happens early, they will be tall in pubescent years but shorter than projected in adulthood, due to early closure of the bone growth plates.
If the growth spurt and puberty happen late, they will be short in pubescent years but taller than projected in adulthood, due to a prolonged growth period before closure of the bone growth plates.
These days, x-rays can give a little better estimate by visualizing the growth plates and reading the “skeletal age,” which takes into account the child’s maturity level as described by the Tanner Scales.
That is why I said that the timing of puberty (Tanner stages) is more related to bone age than to chronological age.
Maturation
Puberty is what most people discuss when they talk about a child maturing, and they most often are referring only to the physical changes which are measurable on the Tanner Scale. The discussion needs to go deeper however; because boys’ and girls’ bodies grow not only physically different, but at different timings and different rates and in different orders as well.
Additionally, it’s not only bone and skin that grows. The neurons in the brain change too, leading to all kinds of different thoughts and behaviors and attitudes. We’ll discuss these aspects in the next three parts of this series, which will cover the girls, boys and psychological aspects of “coming of age.”
9 Posts in Puberty Talk (tanner) Series
- Boys Underwear: Boxers, Briefs or Commando - explanation, recommendations – 22 Sep 2018
- FAQ - Boxers, Brief's or Commando – 28 Aug 2018
- Doctor's Talking About Puberty and Sex to Patients – 28 Aug 2017
- Puberty: Psychological Stages - Part 2 – 13 Aug 2015
- Puberty: Psychological Stages – 5 Aug 2015
- Tanner Stages - Boys – 28 Jul 2015
- Tanner & Growth - Girls – 20 Jul 2015
- Tanner Stages and Growth – 12 Jul 2015
- Puberty, Tanner Series: Intro/Index – 11 Jul 2015
Advertisement by Google
(sorry, only few pages have ads)